Digital stimulation
Digital stimulation works by triggering reflexive activity in the upper motor neurone (UMN) bowel to initiate contractile actions in the rectum. Promoting relaxation of the bowel sphincter further assists in bowel emptying.
Please consider the person’s individual needs when planning any bowel procedures. Additional considerations may include previous personal experiences, education provided on the procedure and the person’s level of sensation or ability to feel the procedure.
Preparation
- Prepare and set out the required equipment in advance:
- Non-sterile gloves
- Apron
- Water-based lubricant
- Protective pad (commonly known as a ‘Bluey’), if required
- Soap and water / wipes (for in bed)
- Plastic bag/bin (for rubbish disposal)
- Ensure the individual’s dignity and privacy are maintained at all times.
- Person performing the procedure should introduce themselves, check person’s identification, explain the procedure, and obtain the person’s verbal consent. (Make it clear that the person can request to stop the procedure immediately, if they wish).
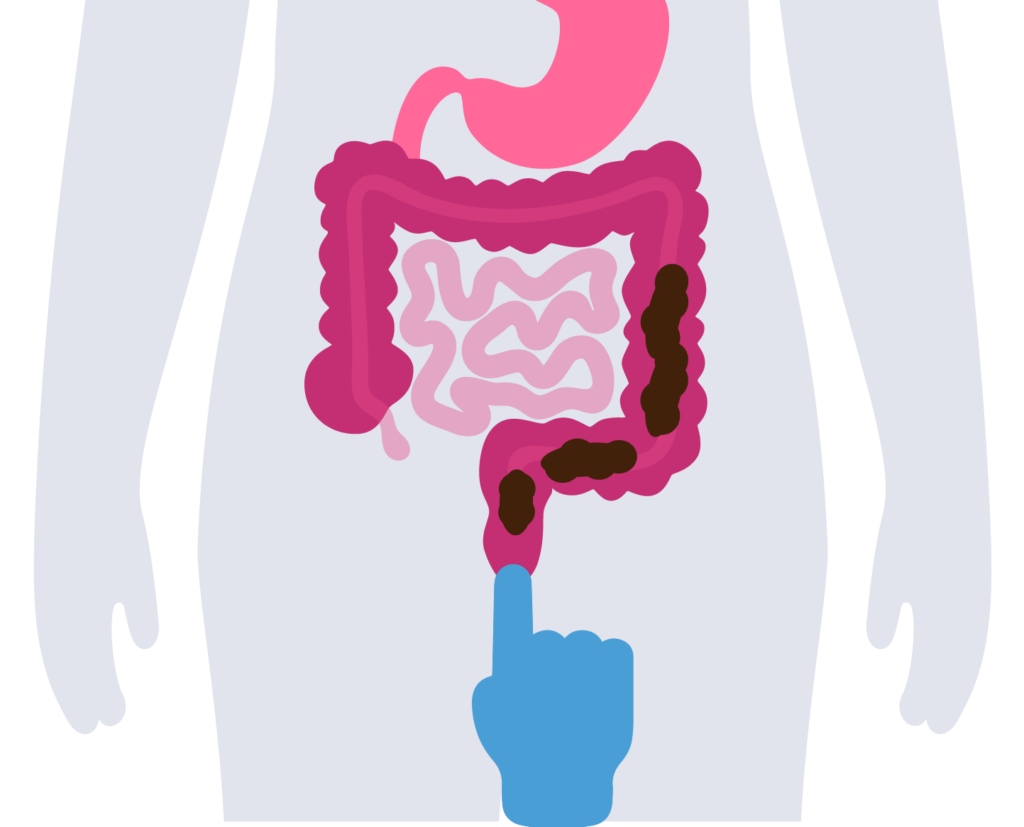
If the faeces are too high in the bowel, it is unlikely to have a result at the time when sitting over the toilet.
If unstable injury
- Procedure needs to take place during formal ‘log roll’ procedure.
- Ensure that correct positioning of the person, such as spinal alignment, is always maintained.
If stable SCI
- Procedure can take place in bed.
- Place person in left lateral position (if possible), flexing the knees to promote stability and expose the anus.
If procedure taking place in shower commode
- Position for comfort and anal access.
- Consider additional needs for safety, such as positioning to ensure anal skin is not stretched during the procedure, using a chest strap in situ and/or using a tilt on the commode chair.
If known to suffer discomfort or signs/symptoms of AD
Local anaesthetic gel may be instilled into the rectum 10 minutes prior to procedure.
- Place protective pad, if required, on the bed of floor of bathroom.
- Wear a plastic apron, wash hands and put on a pair of non-sterile gloves.
- Observe individual throughout procedure (especially those at risk of autonomic dysreflexia (AD)).
- Generously lubricate index finger with water-based lubricant.
Procedure
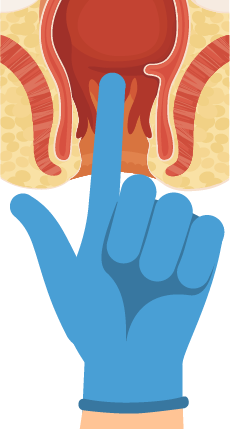
- Inform the person that the procedure is about to begin, then slowly and gently insert a single lubricated, gloved finger 2-4cm into the rectum (this relaxes both the internal and external sphincters) and perform a digital check for faeces.
- If stool is present: gently rotate the straight finger in a circular motion against the rectal wall for approximately 10-20 seconds.
- When the faeces start to move, apply a gentle stretch to the external anal sphincter, to enable the easy passage of faeces.
- Care should be taken to avoid damage to the rectal mucosa and overstretching of the internal and external anal sphincters.
- If no stool present: withdraw finger and await ‘reflex evacuation’. Await 5-10 minutes between stimulation and perform no more than 3 times.
- The presence of mucous (a clear, jelly-like substance) from the lower bowel may be an indicator that the lower bowel is empty – in this case, ongoing stimulation isn’t recommended.
- If the rectal vault feels bulbous (like a blown-up balloon) this could indicate the stool is higher in the bowel and recurrent stimulation is not recommended. Consider dietary and pharmaceutical options to help the stool to move lower down in the bowel.
- Dispose of faecal matter in appropriate receptacle.
- Remove gloves and apron, discard accordingly and perform hand hygiene.
- Apply non-sterile gloves to clean and dry person’s buttocks and anal area.
- Reposition person, if required, and perform hand hygiene.
- Record outcome; such as the amount and consistency of stool (as per the Bristol Stool Scale). See Right consistency for further guidance.
- Report any abnormalities to the person, team leader or medical officer and document accordingly.
- If bleeding or pain is experienced during or after this procedure, please seek medical advice.
- Autonomic dysreflexia may be triggered by this procedure. (See Information on Autonomic Dysreflexia for further guidance).
- Monitor for symptoms and cease stimulation immediately.
As the defecation reflex centre is ineffective for people with LMN bowel types, there is little point in trying to ‘stimulate’ this reflex with the use of enemas, suppositories or digital stimulation (although enemas may provide some level of lubrication to assist in bowel emptying).
The recommended method of evacuating faeces from the rectum for people with LMN bowels is digital removal of faeces (DRF) (formerly referred to as manual evacuation).

Gently rotate the straight finger in a circular motion against the rectal wall for approximately 10-20 seconds.
When you feel the faeces starting to move, apply gentle stretch to the external anal sphincter to enable passage of faeces.