Penile function
Changes in sexual function
The physical aspects of sexual function can change after a spinal cord injury, and these changes depend on the level and type of injury. Some common changes that may occur include:
- Altered sensation that can affect sexual arousal and pleasure.
- Changes in genital arousal, such as differences in how erections occur.
- Difficulty reaching orgasm, or changes in how orgasm is experienced.
- Risk of autonomic dysreflexia during sexual activity or orgasm for people with SCI at or above the level of T6.
- Pain during sexual activity which may result from changes in sensation, positioning, or underlying health issues.
- Problems with ejaculation, such as difficulty ejaculating (ejaculatory dysfunction) or absence of ejaculation (anejaculation).
- Differences in the direction of ejaculation, such as forward (antegrade), backward into the bladder (retrograde), or absent.
- Priapism (a prolonged erection) may occur during the spinal shock phase, especially in injuries at or above T6.
Erectile function after spinal cord injury
SCI can affect how erections occur. There are two main types of erections:
Reflex erections
- Triggered by physical stimulation (touch).
- More likely in people with injuries at the level of T12 and above (upper motor neuron injuries).
Psychogenic erections
- Triggered by erotic thoughts or sensory stimuli (such as visual, auditory, or olfactory cues).
- More likely in people with injuries below T12 (lower motor neuron injuries).
Note: The ability to achieve reflex or psychogenic erections varies depending on individual factors such as the level and completeness of injury, and any other health conditions that affect vascular or neurological function. It is important that individuals discuss their specific circumstances with their healthcare specialist, to explore the most appropriate options for supporting their erectile function and overall sexual health.
Erectile dysfunction
Erectile dysfunction is a common change in sexual function that can happen after a spinal cord injury (SCI). In some cases, a person may have already experienced erectile dysfunction before their injury due to:
- Certain medications or substances (like opioids, antidepressants, or alcohol).
- Health conditions (such as thyroid problems, low testosterone or prolactin, heart or blood vessel issues, diabetes, or prostate removal).
Treatment options for erectile dysfunction
There are several ways to manage erectile dysfunction, and the best option depends on the individual. A collaborative, person-centred approach is key, and it is advisable to refer to or consult with clinicians experienced in sexual health or neurogenic sexual function.
Possible options include:
- Oral medications
- Injectable medications
- Mechanical devices – such as pumps or constriction bands
- Implants – surgically placed devices (considered with caution due to specific risks)
Funding options may be available for some devices or medications. Encourage individuals to check with their funding body or insurer.
Oral medications
Phosphodiesterase type 5 (PDE5) inhibitors (e.g., sildenafil, tadalafil, vardenafil, avanafil) are a group of medications commonly used to treat erectile dysfunction. These medications, sometimes referred to as vasodilating drugs:
- enhance blood flow to the penile tissue
- vary in timeframes for onset and duration
- may cause side effects such as headache, nausea, hypotension, and dyspepsia (indigestion).
Vasodilating drugs should not be used in conjunction with nitrates, such as glyceryl trinitrate (GTN), as they can further lower blood pressure. Nitrates are used to treat autonomic dysreflexia and can also be found in some haemorrhoid creams.
Injectable medications
Injectable options contain alprostadil, which is administered directly into the corpus cavernosal tissue (erectile tissue). This can be an effective treatment for erectile dysfunction, considered where oral medications are ineffective, poorly tolerated or contraindicated.
Health professionals should:
- Provide formal training on injection technique, ideally through a specialised clinic. This training can be provided at the Spinal Injuries Outpatient Sex & Fertility Clinic, which requires a GP referral.
- Assess the individual’s ability to safely inject the drug themselves, or with assistance from a partner.
- Educate the individual on:
- The need to slowly increase the dose in collaboration with the prescribing clinician.
- Frequency limits (maximum once per day, up to three times weekly).
- Possible side effects and risks include: penile pain, bleeding, hypotension, prolonged erections (including priapism), and fibrosis of the penile tissue, with increased frequency of injections.
- Contraindications: Injectable medications should not be used in conjunction with anticoagulant use, sickle cell anaemia or trait, leukaemia, multiple myeloma, or hypersensitivity to alprostadil.
Mechanical devices
Pumps, or vacuum erection devices are an option to be utilised where medications are ineffective, poorly tolerated or contraindicated. When discussing this option with individuals, highlight the following considerations:
- The mechanism draws venous blood into the penis, which may alter its appearance.
- Pumps are typically used in conjunction with constriction bands.
- Choose adjustable bands made of elastic or silicone material, to minimise the risk of pressure injuries.
- Avoid metal or rigid bands as they increase the risk of skin trauma.
- Follow recommended time limits for band use (usually no more than 30 minutes), as prolonged constriction increases injury risk.
- Monitor skin integrity during and after use to promptly address any signs of pressure injury or skin breakdown.
- Water-based or silicone lubricants are recommended to minimise friction during use.
- A “hinging” effect at the base of the penis may occur; instruct the person to use the device gently—particularly if there is reduced or absent sensation.
- Contraindications: Avoid use of mechanical devices in individuals on anticoagulants or those with sickle cell anaemia.
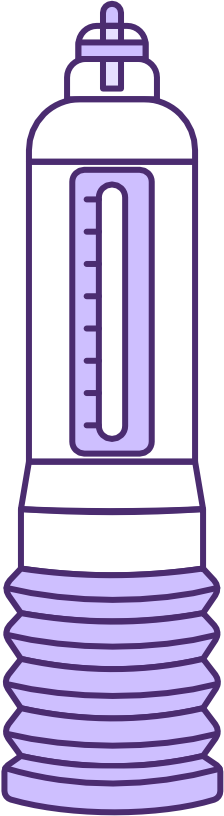
Example of mechanical device
Source: Hydromax by Bathmate
Example of mechanical device
Source: Vacurect

Example of mechanical device
Source: Timm Medical Technologies
Implantable devices
Surgically implanted devices, known as penile prostheses are an option that require further counselling due the higher risk associated with this procedure.
Where this option is being considered, initial consultation with a spinal cord injuries rehabilitation consultant or urologist specialising in this area is essential. Information can be provided through the Spinal Injuries Outpatient Sex and Fertility Clinic. A GP referral is required.
Sexual and reproductive health following spinal cord injury
SCIRE Professional: Spinal Cord Injury Research Evidence
Sexuality following spinal cord injury
New South Wales Government Agency for Clinical Innovation (NSW ACI)
Sexuality and reproductive health in adults with spinal cord injury: what you should know
Consortium for Spinal Cord Medicine
SCI sexual health
Spinal Cord Injury British Colombia (SCI BC)
Sexuality after spinal cord injury
Mount Sinai Hospital
Sexuality and sexual functioning after SCI
Model Systems Knowledge Translation Centre (MSKTC)
Sexuality and fertility following spinal cord injury
Spinal Cord Injuries Australia (SCIA)
Sex and fertility information
Facing Disability for families facing spinal cord injury
Social work and psychosexual therapy resources
Care Rehab
Understanding sexual dysfunction in spinal cord injury
Mens Health Downunder
Agency for Clinical Innovation. (2017). Fertility following spinal cord injury. NSW Government. https://aci.health.nsw.gov.au/__data/assets/pdf_file/0006/600855/ACI-Fertility-following-spinal-injury.pdf
Agency for Clinical Innovation. (2014). Sexuality following spinal cord injury: A guideline for health professionals. NSW Government. https://aci.health.nsw.gov.au/__data/assets/pdf_file/0004/349051/ACI-Spinal-sexuality-guideline.pdf
Alexander, M., Courtois, F., Elliott, S., & Tepper, M. (2017). Improving Sexual Satisfaction in Persons with Spinal Cord Injuries: Collective Wisdom. Topics in spinal cord injury rehabilitation, 23(1), 57-70. https://doi.org/10.1310/sci2301-57
Bryant, C., Aplin, T., & Setchell, J. (2022). Sexuality Support After Spinal Cord Injury: What is Provided in Australian Practice Settings? Sexuality and Disability, 40(3), 409-423. https://doi.org/10.1007/s11195-022-09756-w
Bryant, C., Gustafsson, L., Aplin, T., & Setchell, J. (2021). Supporting sexuality after spinal cord injury: A scoping review of non-medical approaches. Disabil Rehabil, 44(19):5669-5682. https://doi.org/10.1080/09638288.2021.1937339
Earle, S., O’Dell, L., Davies, A., & Williams, R. (2020). Views and experiences of sex, sexuality and relationships following spinal cord injury: A systematic review and narrative synthesis of the qualitative literature. Sexuality and Disability, 38(4), 567–595. https://doi.org/10.1007/s11195-020-09653-0
Elliott, S., Hocaloski, S., & Carlson, M. (2017). A Multidisciplinary Approach to Sexual and Fertility Rehabilitation: The Sexual Rehabilitation Framework. Topics in spinal cord injury rehabilitation, 23(1), 49-56. https://doi.org/10.1310/sci2301-49
Elliott, S., & Querée, M. (2018). Sexual and reproductive health following spinal cord injury. In J. J. Eng, R. W. Teasell, W. C. Miller, D. L. Wolfe, A. F. Townson, J. T. C. Hsieh, S. J. Connolly, V. K. Noonan, E. Loh, S. Sproule, A. McIntyre, & M. Querée (Eds.), Spinal cord injury rehabilitation evidence (Version 6.0, pp. 1–133). SCIRE Project. https://scireproject.com/wp-content/uploads/2022/04/SCIRE-Sexual-Health-Version-6-chapter_Nov.23.18-v.FINAL-2.pdf
Lynch, C., & Fortune, T. (2019). Applying an Occupational Lens to Thinking About and Addressing Sexuality. Sexuality and Disability, 37(2), 145-159. https://doi.org/10.1007/s11195-019-09566-7
Henke, A. M., Billington, Z. J., & Gater, D. R., Jr (2022). Autonomic Dysfunction and Management after Spinal Cord Injury: A Narrative Review. Journal of personalized medicine, 12(7), 1110. https://doi.org/10.3390/jpm12071110
Paralyzed Veterans of America. (2012). Sexuality and reproductive health in adults with spinal cord injury: A clinical practice guideline for health care professionals. https://pva.org/wp-content/uploads/2021/09/sexuality-consumer-cpg-2012.pdf
Taylor, B., Davis, S. The Extended PLISSIT Model for Addressing the Sexual Wellbeing of Individuals with an Acquired Disability or Chronic Illness. Sex Disabil 25, 135–139 (2007). https://doi.org/10.1007/s11195-007-9044-x