Surgical options for bladder management
Below is a list of surgical procedures that may be performed to manage detrusor overactivity and bladder sphincter dysfunction. This is not a complete list and it is best to discuss any procedures with a urologist or spinal cord injury rehabilitation specialist. Individuals can be referred to the Spinal Injuries Unit outpatient clinic for further assessment and discussion regarding surgical options.
Sphincterotomy
A sphincterotomy is the transurethral resection of the external urethral sphincter. It requires the use of an external drainage device called a urinary sheath. The use of an external device means it is only used for males. This procedure is not performed often due to the following:
- The need for repeated procedures to maintain patency
- Incomplete emptying
- Detrusor changes from bladder distension
- Potential ureteric reflux
- Skin irritation from sheath usage
- Challenges with application of the sheath due to reduced penile length
- Risk of outlet obstruction
Mitrofanoff
The Mitrofanoff surgery involves the appendix being used to divert urine from the bladder through the abdominal wall, often at the umbilicus. This allows the person to pass an intermittent catheter through the umbilicus, directly into the bladder. This method of bladder management can be discreet, and can be easier for some individuals to perform. It can be combined with a bladder augmentation, which is outlined further below. The principles of intermittent clean self catheterisation (ICSC) should be adhered to.
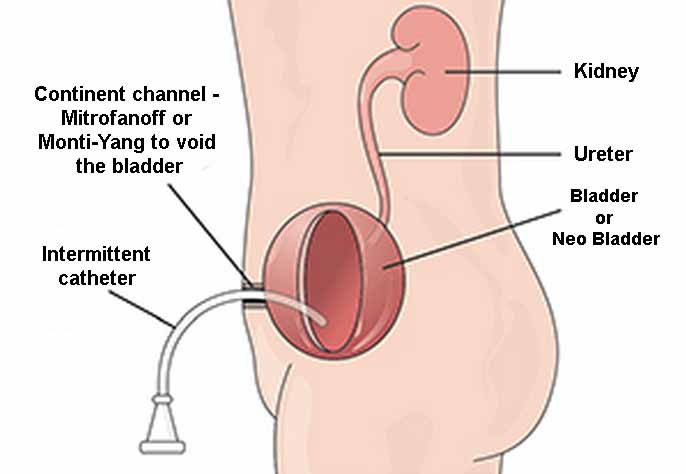
Mitrofanoff surgical procedure. Figure sourced from: Queensland Stoma Association
Bladder augmentation
Bladder augmentation is a procedure which increases bladder capacity. It is usually considered when conservative approaches to managing detrusor overactivity have failed and there is ongoing incontinence or deterioration in renal function. One method is the ‘clam-shell’ ileocystoplasty, where the bladder is opened like a clam and an isolated segment of small intestine (ileum) is used to create a patch that is then sewn into the bladder. A bladder augmentation can lead to an increase in bladder mucous which continues to be produced by the small . To manage the mucous, the person may need to attend frequent high-volume bladder washouts. This procedure is outlined in the bladder washout procedure.
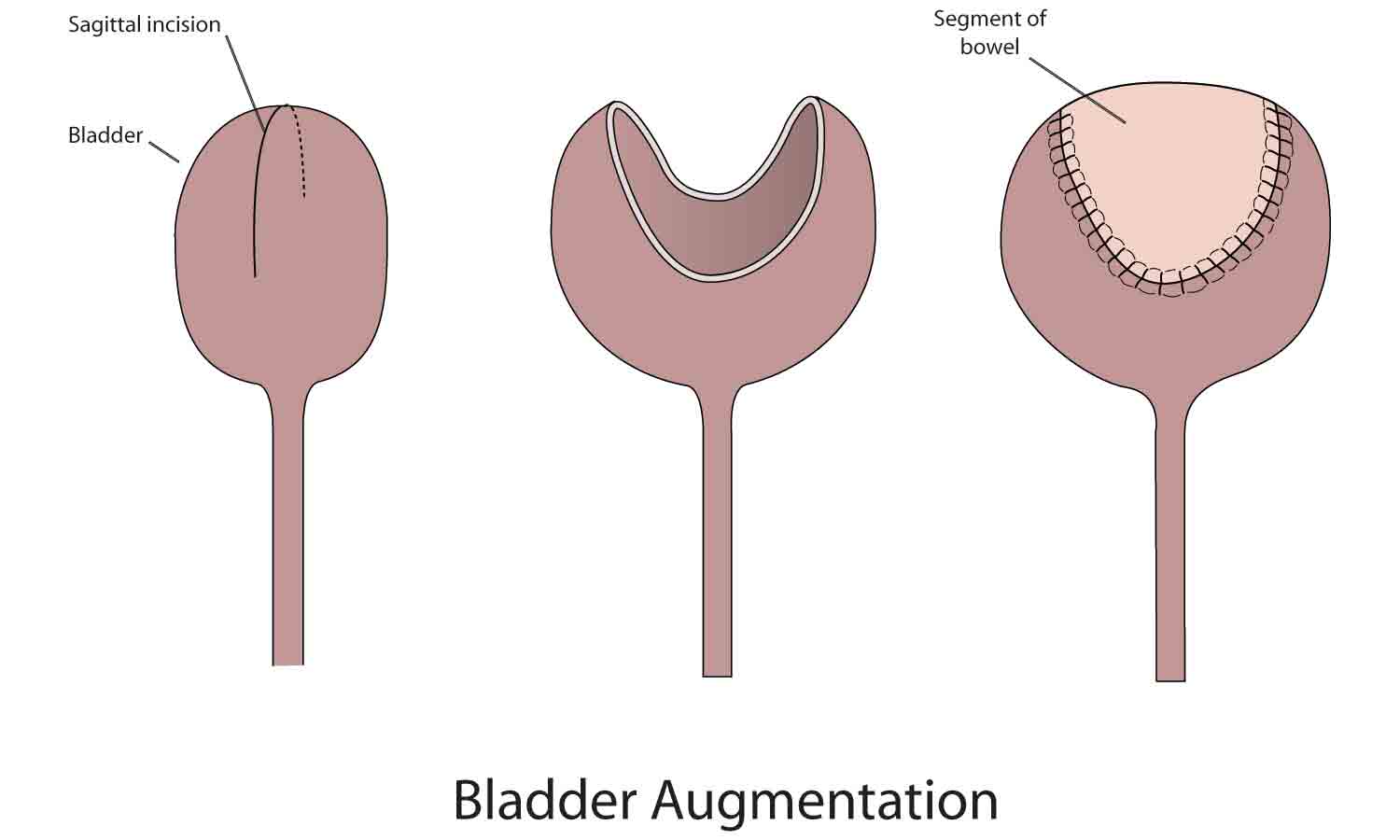
Bladder augmentation surgical procedure steps. The segment of bowel used for the procedure is often from the ileum. Figure sourced from: Model Systems Knowledge Translation Center
Artificial urinary sphincter
An artificial urinary sphincter is an implantable device for males that addresses urethral leaking. Urethral leaking is a common complication following lower motor neuron injuries (for example: cauda equina) and mixed upper and lower motor neuron injuries (for example: conus medullaris injuries). Risks associated with this method of bladder management include device failure, infection and erosion of surrounding tissue.
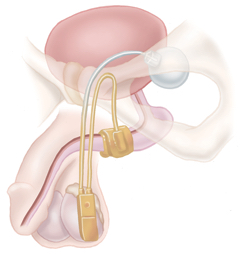
An artificial urinary sphincter. The artificial sphincter wraps around and closes off the urethra. It is activated by a pump in the scrotum.
Mid-urethral sling
A mid-urethral sling is performed to address stress urinary incontinence in women, which is common after SCI due to pelvic floor dysfunction. A mid-urethral sling helps re-establish the position of the urethra, achieve urethral closure and stop ongoing urinary leakage.
Generic information on stress urinary incontinence and treatment options can be found here.
Ileal conduit
An ileal conduit (also known as a bladder stoma or urostomy) involves a section of the small intestine (the ileum) being used to divert urine from the ureters to the outside of the abdomen, where it drains into a bag. This method of bladder management means the bladder is no longer used or connected. The bladder can be left in place or removed, and is determined by the surgeon. Indications for an ileal conduit include ongoing urinary leakage, sphincter dysfunction or renal complications. If the bladder remains in place, a bladder washout will need to be performed regularly.
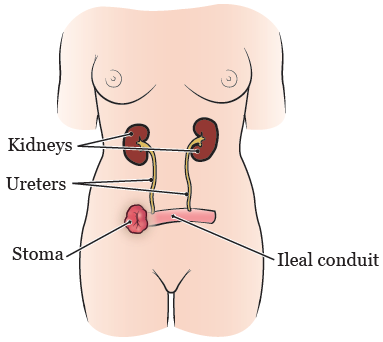
An ileal conduit. Figure sourced from: Memorial Sloan Kettering Cancer Center